Appendix
Neuropsychological Tests
A large number of neuropsychological tests are commercially available. Many more, designed initially by psychologists for their own clinical or research purposes, or both, have become fairly widely used, but are not published. In this section, I will describe only a fraction of the tests potentially available. The ones I have chosen to describe are either (i) tests so commonly used by professional neuropsychologists (for example, the Wechsler Intelligence and Memory Scales) that clinicians interested in cognitive function should be aware of their make-up and scoring, if they are going to interpret neuropsychological reports (these tests are, on the whole, fairly time-consuming, and require training in administration, scoring, and interpretation); or (ii) tests that can be regularly used in the clinic or ward, that do not require special training, and that are relatively quick to administer and score (for example, digit span, story recall, Rey figure copy and recall, and letter and category fluency tests). The tests are arranged in alphabetical order. Normative data are given as means with standard deviations (shown as X ± Y). In the case of those tests that are professionally produced and copyrighted, I have given the name of the publishers. The addresses of the major test publishers are listed at the end of the Appendix.
The Autobiographical Memory Interview (AMI) (Pearson Assessment)
The AMI was designed by Kopelman, Wilson, and Baddeley to assess personal remote (retrograde) memory. There are two sections: the personal semantic schedule and the autobiographical incident schedule. In the first section, subjects are asked to recall specified facts from each of three epochs: childhood (for example, names of teachers and school), early adult life (for example, name of first employer, date and place of wedding), and recent life (for example holidays, journeys, and hospitalizations). Each of these is scored for detail and accuracy by checking with an informant. The second section assesses remote episodic memory. Subjects are asked to recall three specific incidents from each of the same life-periods. Scoring is in terms of the descriptive richness of the incident and its specificity to place. Normative data are available, with cut-offs for probable and definite impairment on both sections. The interview has been used in amnesic and demented patients.
Behavioural Assessment of the Dysexecutive Syndrome (BADS) (Pearson Assessment)
This battery was developed by Barbara Wilson and colleagues to predict and measure everyday problems arising from dysexecutive syndromes. It was hoped that it would overcome deficiencies associated with previous tests by including tasks specifically sensitive to skills involved in problem-solving, planning, and organizing behaviours over an extended period of time. Several of the subtests are more ecologically orientated than traditional neuropsychological tests and were designed to mimic everyday situations. The overall test battery takes approximately 40–60 minutes to administer and comprises the following subtests:
Also included within the battery is the Dysexecutive Questionnaire (DEX), a 20-item questionnaire constructed in order to sample a range of problems commonly associated with dysexecutive syndromes such as emotional and personality changes, motivational problems, and behavioural changes.
For each test, scores are converted into a profile score with the best being a score of 4 and the worst 0. Extensive normative data on 216 normal subjects in each of three ability bands based on National Adult Reading Test (NART) scores are provided.
The Behavioural Inattention Test (BIT) (Pearson Assessment)
The BIT was developed as a standardized test for detecting and measuring the severity of visual neglect, primarily in stroke and head-injured patients. It has been extensively validated, and normative data exist. It consists of six conventional tests, of which the most sensitive is the Star Cancellation Test, and nine behavioural tests which use everyday situations to judge visual neglect. Normative data are available, and the battery has now been widely used in stroke patients to assess neglect phenomena.
The Boston Naming Test (BNT) (Harcourt Assessment Resources, Inc.)
The BNT consists of 60 line drawings, graded from very familiar, highfrequency items such as bed, tree, and pencil through to low-frequency items such as trellis, palette, and abacus. Adults start with item 30 and proceed forward unless they make mistakes in the first eight items. Standard stimulus cues (for example, pencil ‘used for writing’) and phonetic (first-syllable) cues are given if items are unnamed. The test has been widely used in aphasia studies. Fairly extensive normative data are available. There is also a shortened 15-item version of the test.
California Verbal Learning Test (CVLT and CVLT-11) (Pearson Assessment)
The CVLT is designed to assess the use of semantic associations as a strategy for learning words. Each of the 16 words in the CVLT list belongs to one of four categories of shopping list items: for example, list A, Monday’s list, contains four names of fruits, four of herbs and spices, four of articles of clothing, and four of tools; list B, the Tuesday interference list, also contains the names of fruits and of herbs and spices plus four kinds of fish and four kitchen utensils. Category items are presented in a randomized order with instructions to recall the words in any order, thereby assessing the subject’s spontaneous use of semantic associations. CVLT performance is a measure of the interaction between verbal memory and conceptual ability. The procedure is similar to the older Rey Auditory Verbal Learning Test (see later in this chapter). Following five trials of list A, the interference list B is read to the subject. Two short-delay recalls of list A are obtained. The first of the two recall trials is a ‘free’ recall in which the request for the subject to ‘tell me all’ remembered items from list A is identical to the RAVLT free recall procedure. Immediately following the free recall trial the examiner asks the subject to recall items in each of the four semantic categories (‘cued’ recall). For subjects who use semantic clustering during the learning, cueing at delayed recall offers little additional benefit. However, subjects who fail to make the semantic associations during the learning trial often benefit from cueing. There is then a long delay recall at 20 minutes under the same two conditions, ‘free’ and ‘cued’, followed by a recognition trial in which subjects have to recognize items presented from a mixture of the following categories: list items, non-list items from the presented categories, items bearing a phonetic resemblance to the list items, and items that one might find in a supermarket but were not included in the lists.
In addition to the acquisition scores for trials 1–5, ‘free’ and ‘cued’ recall of list A for short and long delays, the test also allows a number of other scores to be derived including recall consistency, semantic clustering, perseverations, false positives, and intrusions. The CVLT manual provides normative data for 273 males and females in seven age-bands covering ages 17–80 years. The CVLT has been shown to be sensitive to memory problems in early Alzheimer’s disease, Parkinson’s disease, frontal lobe disorders, multiple sclerosis, and a range of other forms of organic brain disease.
Cambridge Neuropsychological Test Automated Battery CANtab (Cambridge Cognition)
The CANTAB battery was originally developed by Sahakian, Robbins, and colleagues in Cambridge. It is administered on a computer screen producing, therefore, both reaction time and error scores. The tests in the battery were derived from findings in non-human primate research in an attempt to develop tasks that were sensitive and specific to focal brain damage. It has been extensively used, particularly in a research setting and more recently in pharmacological studies. There are extensive normative data in more than 2000 subjects covering the age range 4–90 years in four different IQ bands. It now consists of 22 tests, listed as follows:
Cambridge Semantic Memory Test Battery
(This test is available from the author.)
This battery was developed in the early 1990s to assess the status of semantic memory in patients with neurodegenerative disorders and has proven extremely valuable over the years. It has not been formally published. The battery employs a consistent set of stimulus items and is designed to assess input to, and output from, a putative central semantic store of knowledge via different sensory modalities. The original version of the battery was based on 48 items chosen to represent three categories of natural kinds (animals, sea creatures, and birds) and three categories of artefacts (household items, vehicles, and musical instruments) which were matched for prototypicality and word frequency. The subsequent version was modified and extended to increase the number of items to 64 with better matching based upon familiarity and age of acquisition. In the newer version of the battery the natural kinds comprise domestic animals (for the UK), foreign animals, fruit, and birds while the artefacts are large household items, small household items, vehicles, and tools. The following subtests comprise the battery.
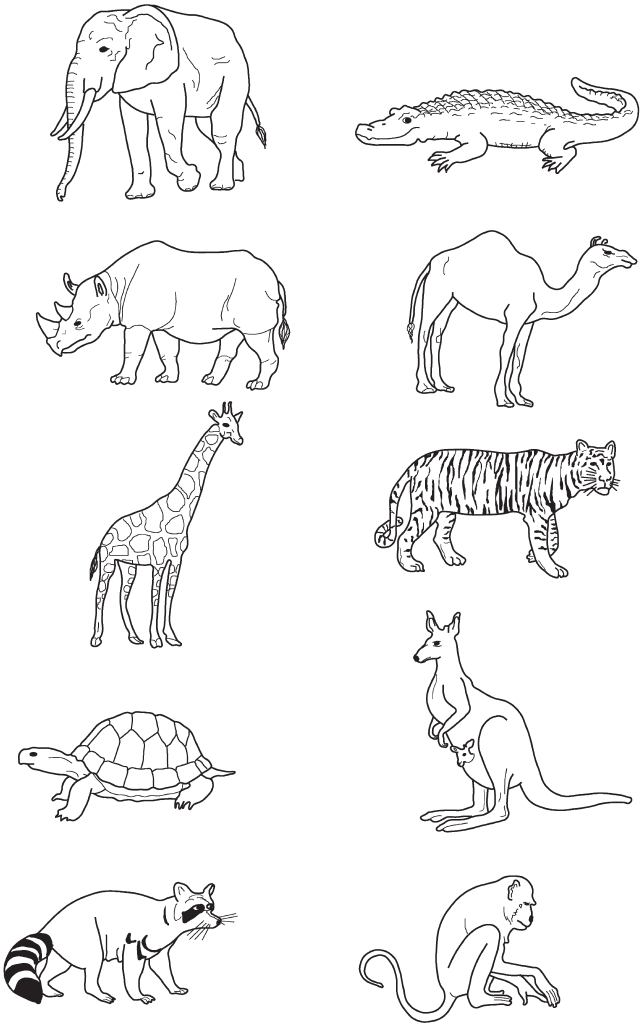
Fig. A.1 Word–picture matching subtest from the Cambridge Semantic Battery.
Our standard assessment battery contains category fluency, naming, word– picture matching, and the Camel and Cactus Test for pictures. The other tests have been used in various research projects. Limited normative data are available. This is clearly a research test battery rather than one applicable for general clinical usage. It is extremely valuable in the assessment of patients with suspected semantic dementia and other rarer disorders involving semantic memory.
Cognitive Estimates Test
In this task, devised by Shallice and Evans, patients are asked to make estimates such as ‘What is the largest object normally found in the house?’ and ‘How fast do racehorses gallop?’. The questions cannot be answered directly from general knowledge. They require novel reasoning, and a comparison with information in the individual’s store of knowledge. Patients with frontal lobe disorders give bizarre answers, when are often not easily modified by asking the patients to reconsider their answers. The specificity and sensitivity of the test have not been well studied, but since there are no good alternative tests it remains clinically useful. A modification of the original test (which contained 15 questions) is given in Table A.1. The test is introduced by saying ‘I’d like you to make the best guess you can in answer to these questions. Almost certainly you won’t know the correct answer, but just make your best guess’. Each answer is scored for unusualness or extremeness. Answers in the correct range score 0. Some responses have to be interpolated, since the scoring system given cannot cover all possibilities.
Table A.1 cognitive estimates Test
| Questions and error scores | Correct range | ||||
|---|---|---|---|---|---|
| 1. What is the height of the London BT Tower? | 100–800 feet | ||||
| > 1500 | 3 | < 60 | 3 | ||
| = 1500 | 2 | = 60 | 2 | ||
| > 800 | 1 | < 100 | 1 | ||
| 2. How fast do racehorses gallop? | 15–40 m.p.h. | ||||
| > 50 | 3 | < 9 | 3 | ||
| = 50 | 2 | < 15 | 2 | ||
| > 40 | 1 | ||||
|
3. What is the best-paid job in Britain today?Manual worker 3Blue-collar worker Professionals 1 |
Queen / film or popstar / sportsman / prime Minister, etc. | ||||
| 4. What is the age of the oldest person in Britain today? | 104–113 years | ||||
| > 115 | 3 | < 103 | 3 | ||
| = 115 | 2 | = 103 | 1 | ||
| = 114 | 1 | ||||
| 5. What is the length of an average man’s spine? | 1′7″–3′11″ | ||||
| > 5′0″ | 3 | < 1′6″ | 3 | ||
| > 4′0″ | 2 | = 1′6″ | 2 | ||
| = 4′0″ | 1 | ||||
| 6. How tall is the average English woman? | 5′3″–5′8″ | ||||
| > 6′0″ | 3 | < 5′2″ | 3 | ||
| = 5′11″, 6′0″ | 2 | = 5′2″ | 1 | ||
| = 5′11″, 5′10″ | 1 | ||||
| 7. What is the population of Britain? | 20–60 million | ||||
| > 1000 million | 3 | < 2 million | 3 | ||
| > 500 million | 2 | < 5 million | 2 | ||
| = 500 million | 1 | < 20 million | 1 | ||
| 8. How heavy is a full pint of milk? | 1–3 lb (17–43 oz) | ||||
| > 3 lb | 3 | < l lb | 3 | ||
| = 3 lb | 1 | = 1 lb | 1 | ||
| 9. What is the largest object normally found in a house? | Bed, bath, etc. | ||||
| < carpet | 3 | ||||
| Carpet | 2 | ||||
| Piano, cupboard, sofa | 1 | ||||
| 10. How many camels are there in holland? | 1–50 | ||||
| Very large number | 3 | ||||
| None | 1 | ||||
| Controls obtain mean error score of 4.0 (± 2.0) | |||||
Adapted from Cortex, 14, 2, Shallice T and Evans M.E., ‘The Involvement of the Frontal Lobes in Cognitive Estimation’, pp. 294–303. Copyright (1978) , with permission from Elsevier
Delis–Kaplan Executive Function System (D-KEFS) (Pearson Assessment)
The D-KEFS is a set of nine tests, each intended to stand alone. The tests were selected to be sensitive to types of executive impairment seen in patients with brain disorders. The subtests comprise trail making, verbal fluency (letter, category, and design fluency), a version of the colour–word interference or Stroop test (see later in this chapter), a sorting test, the 20 questions test, a Tower of London-type test, and a proverbs test. It has the advantage that the tests were all normed on 1750 participants aged 8–89 years and alternative forms are available for some of the subtests. As yet, limited data are available from patient populations.
Digit Span
Digit span is a widely used test of auditory verbal short-term (working) memory. What it measures is more closely related to the efficacy of phonological and attentional processes than to what is commonly thought of as memory (see ‘Short-term (working) memory’ in the ‘Memory’ section in Chapter 1). Variations of the task are included in the Wechsler Memory and Intelligence Scales, in which the administration and scoring methods used to obtain raw scores and age-scaled scores differ slightly.
In clinical practice, the following method is appropriate for determining forward and reverse digit span. For digits forwards, subjects are asked to repeat back progressively lengthening strings of digits in the same order as they are given by the examiner. A practice trial of 2 digits is given, followed by the progressively lengthening strings as shown. It is important that the digits are read at one per second without clustering. Two different series are given for each string-length. If the subject passes the first or the second, the next length is given. If both are failed, the test is discontinued. The score is the longest series correctly repeated. For reverse digit span, exactly the same method is used, except that the subject is asked to repeat back the digits in reverse order. Again a trial of 2 digits is given initially (see Table A.2).
The normal range for digits forwards is 6 ± 1. Even this simple test is affected by age and educational level. Spans of 6 or better are within normal limits; a span of 5 may be marginal or normal, depending on the age and education of the subject; a span of 4 is definitely borderline or impaired; and a span of 3 is always defective. Reverse digit span is 5 ± 1. Hence a reverse span of 3 is borderline or defective, depending upon age and education, and 2 is always defective. In any individual, the difference between forward and backward digit span should not exceed 2.
Table A.2 digit span
| Digits forwards | Digits backwards | ||
|---|---|---|---|
| 9–7 | 2 | ||
| 4–1 | 2 | ||
| 4–8–1 | 3 | 6–2 | 2 |
| 6–3–2 | 3 | 1–9 | 2 |
| 6–4–3–9 | 4 | 2–8–3 | 3 |
| 7–2–8–6 | 4 | 4–1–5 | 3 |
| 4–2–7–3–1 | 5 | 3–2–7–9 | 4 |
| 7–5–8–3–6 | 5 | 4–9–6–8 | 4 |
| 6–1–9–4–7–3 | 6 | 1–5–2–8–6 | 5 |
| 3–9–2–4–8–7 | 6 | 6–1–8–4–3 | 5 |
| 5–9–1–7–4–2–3 | 7 | 5–3–9–4–1–8 | 6 |
| 4–1–7–9–3–8–6 | 7 | 7–2–4–8–5–6 | 6 |
| 5–8–1–9–2–6–4–7 | 8 | 8–1–2–9–3–6–5 | 7 |
| 3–8–2–9–5–1–7–4 | 8 | 4–7–3–9–1–2–8 | 7 |
| Forward score | – | Backward score | – |
Digit span is generally vulnerable to focal left hemisphere and frontal lesions. Disorders of attention (for example, delirium or acute confusional states) cause severe reduction, especially in reverse digit span. In Alzheimer’s disease, digit span is well maintained initially but it is reduced in subjects with subcortical dementias.
Doors and People Test (Pearson Assessment)
This test was designed by Alan Baddeley and colleagues to provide comparable measures of visual and verbal memory tested by recall and recognition. It produces scores in normal subjects that avoid floor and ceiling effects and incorporates learning and forgetting measures. It takes approximately 20 minutes to administer and comprises of four subtests—two visual and two verbal:
Normative data are available on 239 subjects stratified in four age-bands from between 16 and 79 years. In addition to raw and age-scaled scores for the four individual tests it is possible to derive composite visual and verbal recall and recognition scores as well as a total memory score and visual–verbal recall discrepancy scores.
The test is used to evaluate patients with suspected episodic memory deficits and is sensitive to early Alzheimer’s disease and to the effects of temporal lobectomy.
The Graded Naming Test (GNT) (Cambridge Cognition)
This was designed by McKenna and Warrington to be a stringent test of naming ability, sensitive to mild degrees of anomia. It consists of 30 line drawings, ranging from low frequency (for example, kangaroo, scarecrow, and buoy) to very low frequency (for example, centaur, mitre, and retort). Some examples are shown in Fig. A.2. Expected scores, based on the WAIS Vocabulary and reading ability, can be calculated. Detailed normative data are available.
Hayling and Brixton Test (Pearson Assessment)
These tests were developed by Burgess and Shallice to assess aspects of frontal executive function: the ability to inhibit a prepotent response (Hayling) and concept formation (Brixton). The Hayling sentence completion test consists of two sections, each comprising 15 sentences which are missing the last word, such as ‘The old house will be torn ...’. The examiner reads aloud each sentence to the subject who is required to make a verbal response. In section one, the subject is asked to complete the sentence sensibly as quickly as possible. In section two, the subject is asked to give a word that is unconnected to the sentence in every way. For example ‘The captain wanted to stay with the sinking ... light bulb’. This test is based on the ability of normal subjects to inhibit a prepotent response.
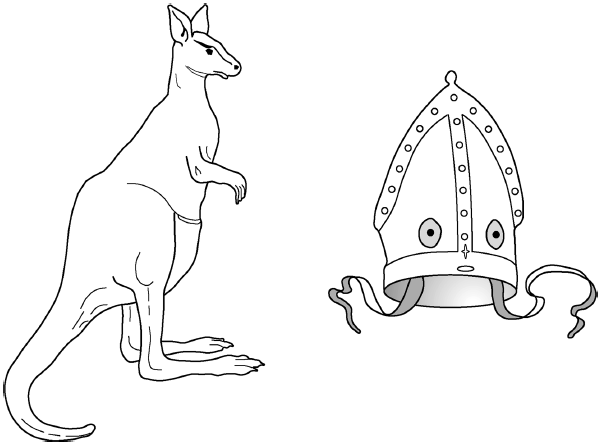
Fig. A.2 Graded Naming Test: an example of one of the easier (kangaroo) and one of the harder (mitre) items from the test.
Reprinted by permission of Cambridge Cognition.
The test yields three measures. The first is the sum of the response latencies in section one. Section two yields two measures of response suppression comprising the time taken and the number of errors. Each response in section two is classified as falling into one of three categories: the first is where the word produced is completely unconnected to the sentence, as required (this scores zero error points); the second type of response is one which is somewhat connected in meaning to the sentence but not a direct sentence completion; the third type of response is where the subject completes the sentence in an entirely plausible fashion. Control data are available for 120 healthy volunteers. It has been shown to be sensitive to unilateral and bilateral frontal lobe damage as a result of structural brain injury and has been applied to patients with frontotemporal dementia.
The Brixton test measures the ability to detect rules in sequences of stimuli and concept formation. It comprises 56 nearly identical cards printed with 10 (2 rows of 5 each) circles, one of which is coloured while the others are white; the position of each succeeding coloured circle is determined by one of nine rules based on the position of the coloured circles on preceding cards (see Fig. A.3). On being told that the coloured circle ‘moves around according to various patterns that come and go without warning’, the subject is asked to state the expected position of the coloured circle on the next card. For the first and simplest rule the coloured circle advances one position clockwise on successive cards and a later rule has the circle alternating from place 5 to place 10. Limited normative data are available but frontal patients are reported to make more errors and to respond in a random and unconstrained fashion.
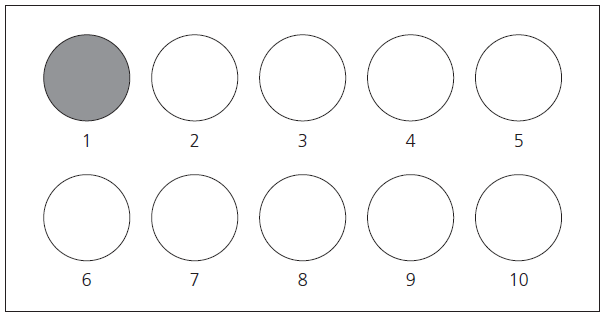
Fig. A.3 Example from the Brixton Spatial Anticipation Test. Hayling and Brixton Tests. Copyright © 1997 by Paul W. Burgess and Tim Shallice. Reproduced with permission of Pearson Education Ltd.
Judgement of Line Orientation Test (JLO) (PAR inc)
This task, designed by Benton and colleagues, examines the ability to judge and match angular relationships. The subject views pairs of lines with various orientations, and is required to estimate their angulation with reference to a display of 11 numbered lines spanning 180 degrees, which are viewed simultaneously with the target lines (see Fig. A.4). The test consists of 30 trials of increasing difficulty. It is quick and easy to administer, and comes with several parallel forms. Reasonable normative data are available. The test is sensitive to focal right parietal lesions. It is also failed consistently by patients with Alzheimer’s disease beyond the earliest stages.
The National Adult Reading Test: Second Edition (NART)
The NART was developed by Nelson and O’Connell as a quick and simple test to estimate premorbid IQ in patients suspected of suffering from intellectual deterioration. The 50 words constituting the NART are all irregular (DEBT, AISLE, DEPOT, THYME, BOUQUET, PLACEBO, etc.), in that they cannot be pronounced correctly by applying the usual rules of spelling-to-sound correspondence. For example, the word NAIVE would be pronounced ‘nave’ if one were to decode it phonetically. The principles underlying the test are (i) that the pronunciation of irregular words depends upon pre-existent familiarity with their meaning; and (ii) that reading is a highly over-learnt skill, which is maintained at a high level despite deterioration in other areas of intellectual functioning.
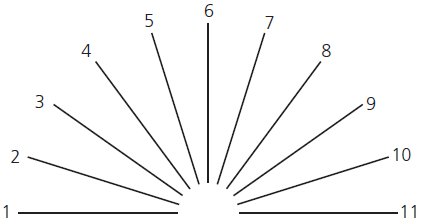
Fig. A.4 Judgement of Line Orientation Test.
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc. (PAR), 16204 North Florida Avenue, Lutz, Florida 33549, from the Judgment of Line Orientation by Arthur l. Benton, PhD, Copyright 1983 by PAR. Further reproduction is prohibited without permission of PAR.
The 50 words of the test are graded in frequency of occurrence in the English language; the initial items (ACHE, DEBT, PSALM) are familiar to the average adult, while the last words (LABILE, SYNCOPE, PRELATE) are beyond most people’s vocabulary. On the basis of the number of errors produced, a premorbid IQ can be estimated in the range 90–128. For subjects below this range the Schonell Graded Word Reading Test should be used. A parallel version, the American National Reading Test (ANART) was developed for an ethnically diverse US population.
While the test remains a valid instrument for estimating premorbid IQ levels in patients with mild dementia, recent research suggests that NART performance declines in moderate Alzheimer’s disease. Patients in whom there is a breakdown of the whole-word (lexical) reading route, surface dyslexics, are particularly impaired at reading irregularly spelt words. Their premorbid IQ should be assessed using other measures, such as Raven’s Matrices, rather than the NART.
Paced Auditory Serial Addition Test (PASAT) (Brain Metric Software)
This sensitive test requires the subject to add 60 pairs of randomized digits so that each is added to the digit immediately preceding it. For example, if the examiner reads the numbers ‘2–8–6–1–9’, the subject correct response beginning as soon as the examiner reads 8 are ‘10–14–7–10’. The digits are presented at four rates of speed each differing by 0.4 seconds and ranging from one every 1.2 seconds to one every 2.4 seconds. The performance can be evaluated in terms of the percentage of correct responses or the mean score for all trials. It is a difficult task and performance declines with age. It has been found to be particularly sensitive to brain trauma following head injury interpreted as reflecting abnormally slowed information processing. The test is experienced as stressful and is typically only given to high-ability subjects to detect subtle attentional deficits.
Pyramids and Palm Trees Test (Pearson Assessment)
This test, devised by Howard and Patterson, assesses a person’s ability to access detailed semantic knowledge from words and from pictures. It can be given in several formats (picture–picture, word–word, picture–word), but the picture– picture-matching version is perhaps the most useful since it assesses non-verbal semantic knowledge. There are 52 items in the test. The subject is presented with three pictures on a single card (see Fig. A.5), the target picture is displayed at the top. The subject has to decide which of the two lower pictures is most closely associated with the target. Examples include an Egyptian pyramid with a fir tree and a palm tree (hence the name of the test); spectacles with eye and ear; and saddle with goat and horse. The test remains largely a research tool, but its usage is likely to increase, since there are few good alternatives. Normative data are, at present, rather limited. Normal controls make three or fewer errors on the picture–picture-matching version; patients with semantic memory impairment make considerably more.

Fig. A.5 Pyramids and Palm Trees Test: A and B are two examples from the test. Copyright © 1992 by David Howard and Karalyn Patterson. Reproduced with permission of Pearson Education Ltd.
Raven’s Progressive and Coloured Progressive Matrices (Harcourt Assessment Resources, Inc.)
Raven’s Progressive Matrices (RPM) was developed as a ‘culture-fair’ test of general intellectual inability, although it has subsequently emerged that educational level has a major effect on normal subjects’ performance. It consists of 60 visually based problem-solving tests arranged in blocks of increasing complexity. The initial test items require only pattern matching; the subject is faced with a large design, part of which is missing; below are six different small pattern-samples, one of which the subject chooses to complete the larger design above. As the test progresses, the items become more complex, requiring reasoning by analogy rather than simple pattern matching. The test is simple to administer, but takes 45 minutes or so to complete. Detailed normative data with percentile scores are available for ages 8–65 years.
Raven’s Coloured Progressive Matrices (RCPM) provide a simplified 36-item format, with norms for children and adults aged over 65 years. It has also been used in neuropsychological practice. A greater proportion of the test items are of the pattern-matching type than in the RPM.
Both tests are sensitive to brain damage in fairly widely distributed areas, since normal performance depends upon intact visuoperceptual, attentional, and problem-solving skills. In the absence of visuoperceptual deficits it is a reasonable test of frontal lobe function.
Recognition Memory Test (RMT) (Pearson Assessment)
This easy-to-administer test of word and face recognition memory was devised by Warrington. In the face memory part, the subject is shown 50 black-and-white photographs of unfamiliar male faces. The examiner asks the subject to attend to each for 3 seconds and to say whether the faces are pleasant or not. After viewing all 50 faces, subjects are then shown pairs of faces, one of which was in the original series. In this forced-choice recognition format, the subjects have to choose which one they have already seen. The word memory part of the test is given with identical instructions. The subject views 50 high-frequency words, and then has a two-choice recognition test. Normal subjects perform very well on both parts of the test. Good age and IQ-standardized normative data are available, including the acceptable range for a discrepancy between word and face recognition. The test is sensitive to episodic memory disorders and has the advantage of containing verbal and non-verbal tasks in the same format.
Rey Auditory Verbal Learning Test (RAVLT)
This is a verbal serial learning test using 15 common nouns. It provides a measure of immediate recall, evaluates learning over successive trials, and assesses confabulation and susceptibility to interference.
Five presentations of one list (A) are given, then one presentation of the second list (B), followed by a sixth recall trial of list A (see Table A.3). The examiner reads list A at one word per second, after giving instructions along these lines: ‘I am going to read you a list of words. Listen carefully, because when I stop you will have to repeat back as many as you can. It doesn’t matter in what order you repeat them’.
Table A.3 Rey Auditory Verbal Learning Test (RAVLT)
| List A | Trials | List B | Trial | |||||
|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | Recall | VI | ||
| 1 Drum | _ | _ | _ | _ | _ | 1 Book | _ | _ |
| 2 Curtain | _ | _ | _ | _ | _ | 2 Flower | _ | _ |
| 3 Bell | _ | _ | _ | _ | _ | 3 Train | _ | _ |
| 4 Coffee | _ | _ | _ | _ | _ | 4 Rug | _ | _ |
| 5 School | _ | _ | _ | _ | _ | 5 Meadow | _ | _ |
| 6 Parent | _ | _ | _ | _ | _ | 6 Harp | _ | _ |
| 7 Moon | _ | _ | _ | _ | _ | 7 Salt | _ | _ |
| 8 Garden | _ | _ | _ | _ | _ | 8 Finger | _ | _ |
| 9 Hat | _ | _ | _ | _ | _ | 9 Apple | _ | _ |
| 10 Farmer | _ | _ | _ | _ | _ | 10 Chimney | _ | _ |
| 11 Nose | _ | _ | _ | _ | _ | 11 Button | _ | _ |
| 12 Turkey | _ | _ | _ | _ | _ | 12 Key | _ | _ |
| 13 Colour | _ | _ | _ | _ | _ | 13 Dog | _ | _ |
| 14 House | _ | _ | _ | _ | _ | 14 Glass | _ | _ |
| 15 River | _ | _ | _ | _ | _ | 15 Rattle | _ | _ |
| Total | _ | _ | _ | _ | _ | _ | _ | _ |
Data from A. Rey L’examen psychologique dans les cas d’encéphalopathie traumatique, Archives de Psychologie, 28 (1941), p. 21
After the first trial the examiner re-reads the same list a total of five times, using the same instructions, but emphasizing that the subject should include words recalled on previous trials. The order of the subject’s responses should be recorded each time. After Trial V of list A, the examiner reads list B and asks for recall of this list only. Finally, following the list B trial, the subject is asked to recall as many words as possible from the original list. This constitutes Trial VI.
Recall of Trial I is largely a measure of short-term (working) memory, and therefore approximates digit span to within one or two points. It varies according to age and education, so that elderly (>70 years) subjects recall 5 (± 1) and young professionals recall 7–8 (± 1.5). Normal subjects show considerable learning across Trials I–V, with a mean increment of 5 or 6 words above their Trial I recall, and relatively little age-variation. A drop of 3 or more words between trials V and VI of list A is regarded as abnormal. Further details are given in Lezak et al.’s book (see ‘Selected Further Reading’).
Like the RMT, the RAVLT test is sensitive to episodic memory disorders. Patients with the amnesic syndrome show reasonable recall on Trial I, but very little learning over successive trials. They are also sensitive to the interference effects of list B, and tend to confabulate, producing items extraneous to either list.
Rey–Osterrieth Complex Figure Test (Pearson Assessment)
The Complex Figure Test can be used to evaluate both visuo-constructional ability and visual memory. Subjects are asked to copy the figure (see Fig. A6) freehand, without time restriction. A note should be made of their general approach to the task and organizational skills. Some examiners use a sequence of different coloured pencils, which they pass to the subject at 30-second intervals; but this is probably unnecessary in ordinary clinical practice. After a delay, typically 30–40 min, subjects are asked to reproduce the figure without prior warning. Some neuropsychologists also test recall after a few minutes’ delay.
Copying skills are severely disrupted by right hemisphere damage, often with a tendency to neglect the left side of the figure. Patients with extensive left hemisphere lesions may also copy the figure in a disorganized, piecemeal fashion and frontal patients tend to draw impoverished figures with perseverated elements.
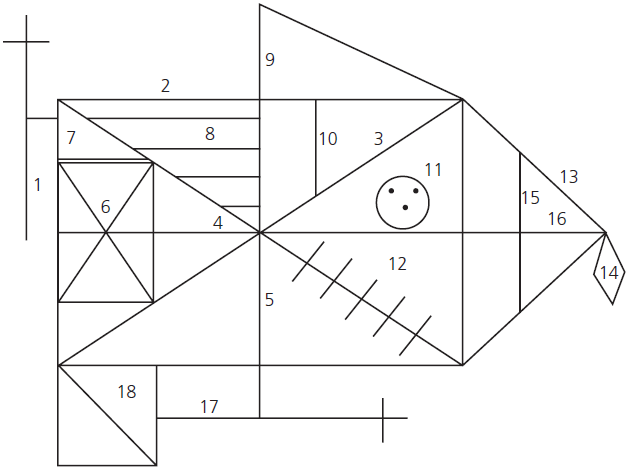
Fig. A.6 Rey–Osterrieth Complex Figure Test. Scoring system.
Recall is very poor in patients with the amnesic syndrome, and with selective right temporal lobe damage. Performance on the copy and recall portions of the test are extremely poor in patients with moderate-to-severe Alzheimer’s disease; but recall is selectively impaired in mild disease.
As well as a qualitative assessment, the accuracy of the copied and recalled versions can be scored using the standardized scoring system shown in Table A.4, which allots a maximum of two points to each of the 18 elements of the figure. Normative data are shown in Table A.5.
Rivermead Behavioural Memory Test: Second Edition (RBMT-II) (Pearson Assessment)
The RBMT was developed initially to assess memory recovery in brain-injured patients. It combines conventional tasks (for example, orientation and story recall) with more real-life tasks (for example, remembering a route and a message) that arguably correlate more closely with psychosocial competence. It is an easy-to-use measure, not requiring special professional training to administer and to score. However, it does take 20–30 minutes to administer. It provides an overall screening score for significant memory impairment, as well as more detailed scores for each of the subtests listed as follows:
Table A.4 Scoring system for Rey–Osterrieth Figure Test
| Scoring system | Score | |
|---|---|---|
| Units | Copy | Recall |
| 1. Cross upper left corner, outside of rectangle | ||
| 2. Large rectangle | ||
| 3. Diagonal cross | ||
| 4. Horizontal midline of 2 | ||
| 5. Vertical midline of 2 | ||
| 6. Small rectangle within 2, to the left | ||
| 7. Small segment above 6 | ||
| 8. Small parallel lines within 2, upper left | ||
| 9. Triangle above 2, upper right | ||
| 10. Small vertical line within 2, below 9 | ||
| 11. Circle with 3 dots within 2 | ||
| 12. Five parallel lines within 2 crossing 3, lower right | ||
| 13. Sides of triangle attached to 2 on right | ||
| 14. Diamond attached to 13 | ||
| 15. Vertical line within triangle 13, parallel to right vertical of 2 | ||
| 16. Horizontal line within 13, continuing 4 to right | ||
| 17. Cross attached to low centre | ||
| 18. Square attached to 2, lower left | ||
| Total | ||
| Placed poorly | Properly placed | |
| Correct | 1 | 2 |
| Distorted or incomplete | 1/2 | 1 |
| Absent or Not recognizable | 0 | 0 |
| Max.: 36 |
Table A.5 Rey–Osterrieth Complex Figure Test normative data
| Normative data | Copy | 30-minute recall |
|---|---|---|
| Adults <60 years | 32 ± 2 | 22 ± 4 |
| Elderly subjects | 28 ± 3 | 13 ± 4 |
Items scored (for RBMT screening score):
| 1. | First name of person in photograph. |
| 2. | Second name (surname) of person in photograph. |
| 3. | Remembering hidden belonging. |
| 4. | Remembering to ask about appointment (question after alarm sounds). |
| 5. | Picture (object) recognition (selecting 10 from 20 shown). |
| 6a. | Prose recall— immediate (21 ideas). |
| 6b. | Prose recall— delayed (20 minutes). |
| 7. | Face recognition (recognizing 5 from 10 shown). |
| 8a. | Route— immediate (five places). |
| 8b. | Route— delayed (about 20 minutes). |
| 9. | Route— message (envelope to be left). |
| 10. | Orientation. |
| 11. | Date (correct). |
Story Recall (Logical Memory)
A number of different paragraph or story recall tests have been used, all of which derive from the Logical Memory Subtest of the Wechsler Memory Scale (WMS), or are modifications of the Babcock story. In the WMS and WMS-R, two stories are used, each containing 25 elements; the score is taken as the mean of those for the two stories. It is usual to test both immediate recall and delayed recall after an interval of 30–45 minutes. The latter has been shown to be particularly sensitive to episodic memory disorders (for example, the amnesic syndrome and Alzheimer’s disease), and to correlate well with real-life memory difficulties. An example is given in Table A.6.
Subjects should be instructed as follows:
‘I am going to read a short story to you now. Listen carefully because when I have finished I am going to ask you to tell me as much of the story as you can remember’. After reading the story, the examiner instructs the patient ‘Now tell me everything you can remember’. Recall is again tested after a delay of approximately 30 min, without prior warning.
Table A.6 Example of a prose passage and age-related norms for recall
| Mary / Allen / of North / Oxford, / employed / as a cook / in a college, / reported / at the police / station / that she had been held up / in Broad Street / that morning / and robbed / of £50. She had three / little children, / the rent was due, / and they had not eaten / for 24 hours. / The officers, / touched by the woman’s story, / made up a purse / for her. [Total elements = 24] |
||||
| Age (years) | ||||
|---|---|---|---|---|
| 20–39 | 40–59 | 60–69 | 70–79 | |
| Immediate recall, mean (SD) | 10.0 (2.5) | 8.0 (2.5) | 7.5 (3.0) | 6.0 (3.0) |
| Delayed recall as % of immediate mean (SD) | 60% (20%) | 55% (20%) | 70% (15%) | 65% (15%) |
A full credit is given for each element of the story recalled correctly. A half credit is given for synonyms, substitutes, or omissions of an adjective or verb that do not alter the basic idea-unit. The test is very sensitive in normal subjects to the effects of age and general intellectual ability. Table A.6 gives a rough guide to the expected normal levels using this test.
Hence, a 60-year-old of high intelligence would be expected to recall more than 10 elements immediately, and to retain at least 60% after a delay. A normal 70-year-old of low intellectual ability could recall as few as 4 elements initially, and retain a third after a delay.
Stroop Tests
These are based on the fact that it takes longer to call out the colour names of coloured patches than to read words, and even longer to name the colour of an ink in which a colour name is printed when the print ink is a colour different from the colour name. The latter phenomenon, a markedly slowed response when a colour name is printed in ink of a different colour, is interpreted as cognitive slowing due to response conflict or a failure of selective attention.
A great number of versions of this test have been published which vary in the number of trials and items. Some formats use only two trials: one in which reading focuses on colour words printed in ink of different colours and the other requiring naming of the colour patches. This includes the popular Dodrill version recommended by Lezak et al. in Neuropsychological Assessment (5th edition). Versions also vary in the number of items in the trial and the number of colours used. A version of the Stroop is included in the D-KEFS test (see earlier in this chapter). The Dodrill version consists of a single sheet containing 176 colour names randomly printed in one of four colours (red, orange, green, blue). In part I, the subject reads the printed word names and in part II the subject reports the colour in which each word is printed (see Fig. A.7). A maximum of 300 seconds are allowed for part I and 600 seconds for part II. Normal controls typically complete part I in around 90 ± 20 seconds and part II in 230 ± 70 seconds. The key score is the difference between parts II and I, which is markedly prolonged in patients with a variety of brain pathologies including epilepsy and early-stage Alzheimer’s disease.
Sydney Language Battery (SYDBAT)
(This test is available from the author.)
The Sydney Language Battery consists of four single-word-based tasks using the same set of 30 stimuli chosen to be of graded difficulty and all comprising items the names for which are multisyllabic: visual confrontation naming, repetition of multisyllabic words, word comprehension, and semantic association. Each task (except the repetition test) is terminated if the subject makes four consecutive errors.
| RED | GREEN | BLUE | BLACK |
| BLUE | PINK | RED | BLACK |
| YELLOW | BLACK | ORANGE | BLUE |
| RED | GREEN | RED | ORANGE |
| GRAY | YELLOW | GREEN | GREEN |
| BROWN | PINK | BLUE | BLACK |
| BLUE | BROWN | YELLOW | BLUE |
| RED | ORANGE | GREEN | RED |
| GREEN | PINK | BLACK | YELLOW |
Fig. A.7 Example of Stroop Test.
Test of Everyday Attention (TEA) (Pearson Assessment)
The Test of Everyday Attention was developed by Ian Robertson and colleagues to evaluate attentional abilities using ecological tasks based upon the subdivision into the following three divisions: selective attention; sustained attention, and attentional switching with the following subtest.
Map search—Subjects have to search for symbols on a coloured map. The score is the number out of 80 found in 2 minutes. This subtest is age sensitive and usable with almost all brain-damaged patients, including those with Alzheimer’s disease. It measures selective attention and loads on the same factor as the Stroop Test and the d2 cancellation test.
Elevator counting—Subjects are asked to pretend they are in an elevator whose door-indicator is not functioning. They therefore have to establish which ‘door’ they have arrived at by counting a series of tape-presented tones. This is an established measure of sustained attention sensitive to right frontal lesions.
Elevator counting with distraction—Subjects have to count the low tones in the pretend elevator while ignoring the high tones. This was designed as a subtest of auditory selective attention.
Visual elevator—Here, subjects have to count up and down as they follow a series of visually presented ‘doors’ in the elevator. This reversal task is a measure of attentional switching, and hence of cognitive flexibility. It is self-paced and loads on the same factor as the number of categories on the Wisconsin Card Sorting Test.
Auditory elevator with reversal—The same as the visual elevator subtest except that it is presented at fixed speed on tape.
Telephone search—Subjects must look for key symbols while searching entries in a simulated classified telephone directory.
Telephone search dual task—Subject must again search in the directory while simultaneously counting strings of tones presented by a tape recorder. The combined performance on subtests 6 and 7 gives a measure of divided attention—a ‘dual task decrement’.
The test has three parallel versions and is sensitive enough to show normal age effects in the normal population.
Test for the Reception of Grammar (TROG-II) (Pearson Assessment)
This test was developed by Bishop for use in children with developmental language disorders but is very useful in the neuropsychological population. It is a sentence–picture matching test that uses low-level vocabulary items (such as horse, boy, or flower) and is cleverly designed to test syntactic comprehension of increasing complexity. Subjects are presented with a page comprising four pictures and are asked to choose the picture which matches the word, or sentence, spoken by the examiner. The early blocks are designed to check comprehension of the vocabulary items. Subsequent blocks increase in complexity such that later trials probe constructions such as embedded clauses and reversible structures. The total possible score is 80. Most normal adults obtain scores in the high 70s, failing occasional items in later complex blocks. By contrast, patients with deficits in sentence comprehension as a result of stroke or neurodegeneration have great difficulty and begin to fail on earlier items in the test.
The Token Test (PRO-ED, Inc.)
The Token Test is a sensitive and reliable measure of auditory comprehension in aphasic stroke patients, although its value in other language-disordered patients is less clear. It is easy to administer and score, and the material needed can be readily made. Twenty ‘tokens’ cut from cardboard, plastic, or wood are used. They come in two sizes: big and small; two shapes: circles and squares; and five colours. The original version consisted of 62 commands, graded from the very simple (for example, ‘Touch the red circle and touch the small green square’) to syntactically complex commands (for example, ‘Put the red circle on the green square’ and ‘Pick up all the squares except the yellow one’).
A shortened version, consisting of 36 commands, has been widely used. Educationally standardized normative data are available.
Trail Making Test
This is a quick and easily administered test of visuomotor tracking, and of conceptualization and mental ‘set shifting’. A version of the trails is included in the D-KEFS battery (see earlier in this chapter). It is given in two parts (A and B). Part A consists of a series of circles enclosing numbers from 1 to 25, scattered at random on the page. The subject’s task is to join the circles in numerical order as quickly as possible. Part B has both numbers and letters arrayed in the random order. The subject must alternate between numbers and letters: 1 to A to 2 to B to 3 to C, and so on to 13.
Various administration and scoring procedures have been used; but it is usual to point out errors as they occur, to allow self-correction, and to score only in terms of time to complete.
In common with any test that depends upon response-speed, performance on trail making depends markedly on age. Approximate age-adjusted upper limits for normality in seconds are given in Table A.7.
Impaired performance on either part of the test can result from motor slowing, incoordination, visual scanning difficulties, poor motivation, or frontal executive problems. Patients with frontal lobe dysfunction perform disproportionately badly on part B.
Verbal Fluency Tests: Letter and Category Fluency
Verbal fluency, sometimes referred to as controlled oral word association, is a very useful bedside test which is sensitive to frontal ‘executive’ dysfunction and subtle degrees of semantic memory impairment. A number of versions based on letter and semantic category have been used. The most extensive experience is of ‘FAS’ for letter fluency, and the category ‘animals’.
FAS: Subjects are asked to list as many words as possible beginning with each of the three letters in turn. One minute is allowed per letter. Subjects are told beforehand that proper nouns (personal and place names) and repetitions of words with different suffixes (find, finder, finding, etc.) are not acceptable.
Table A.7 Age-adjusted upper limits (10th + 25th percentiles) for normality (in seconds) on the Trail Making Test
| Age (years) | |||||
|---|---|---|---|---|---|
| 20–39 | 40–49 | 50–59 | 60–69 | 70–79 | |
| Part A | |||||
| 10% | 42 | 45 | 49 | 67 | 105 |
| 25% | 50 | 59 | 67 | 104 | 168 |
| Part B | |||||
| 10% | 95 | 100 | 135 | 172 | 292 |
| 25% | 130 | 150 | 177 | 282 | 450 |
Animals: Subjects are asked to list as many animals as possible in 1 minute. If this test is given immediately after letter fluency, it is important to point out that the animal names can begin with any letter.
Scores for the total responses, the number of perseverative errors, and other (intrusive) errors can be obtained. For FAS, it is usual to summate across the three letters. Normal subjects should not perseverate or lose set (i.e. revert to a prior letter). Performance depends on age and education. Young professionals should produce in excess of 45 words for FAS and a total of 30 or below is abnormal. The lowest acceptable total for elderly subjects of low educational attainment is around 25 words. Category fluency is usually superior to letter fluency. For the category animals, normal subjects usually produce 20 exemplars. The lower limit of acceptability ranges from 12 to 15, again depending on age and education.
The Visual Object and Space Perception Battery (VOSP) (Pearson Assessment)
This battery of eight visuoperceptual tests was developed, validated, and standardized by Warrington and James. Each subset was developed to focus on one component of visual perception, while minimizing the contribution of other cognitive skills. Most of the tasks are based on prior experimental studies performed by the authors. All are sensitive to right hemisphere damage, and normative values are included with the battery.
An initial simple figure–ground discrimination test screens out patients with severe visual handicap. The battery proper consists of four tests of object recognition and four tests of space perception.
Object recognition
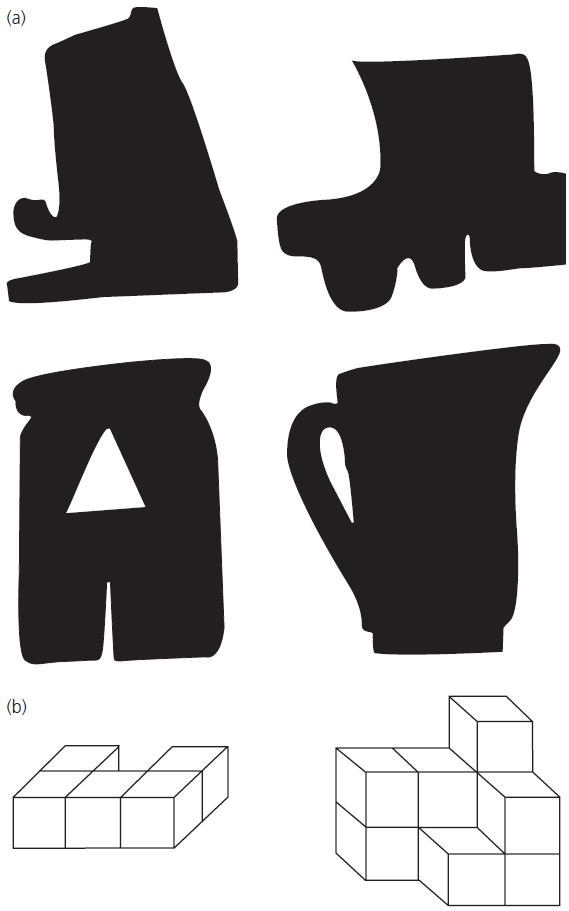
Fig. A.8 Examples of the object decision (A) and cube analysis (B) subtests of the Visual Object and Space Perception Battery.
Copyright © 1991 by Elizabeth K. Warrington and Merle James. Reproduced with permission of Pearson Education Ltd.
Space perception
Wechsler Adult Intelligence Scale (WAIS-R and WAIS-IV) (Pearson Assessment)
The WAIS-R (1981) and the most recently updated version, the WAIS-IV (2008), remain the most widely used test batteries for evaluating general intellectual and neuropsychological ability. For most clinical neuropsychologists, they form the cornerstone of cognitive assessment. A great strength of the WAIS batteries lies in their comprehensive standardization. The WAIS-R included data on 1880 subjects aged 16–87 years and the WAIS-III 2450 subjects aged 16–89 years. A full description of the WAIS-III is beyond the scope of this book. Its administration and scoring are relatively complex and demand formal training. Interpretation of the results depends upon considerable experience. The subject’s behaviour, general approach to testing, and types of errors produced form an important part of the evaluation.
The WAIS-R consists of 11 subtests (six verbal and five performance). The current version of the test, the WAIS-IV, which was released in 2008, is composed of 10 core subtests and five supplemental subtests, with the 10 core tests comprising the Full Scale IQ. By summating the subtest scores and adjusting for age, verbal, performance and full scale IQ scores can be derived. An average person should obtain a score of 100 for each, one-standard deviation being 15 points. In neuropsychological practice, however, the pattern of individual subtest scores is usually more informative than the overall IQ. Each subtest yields a raw score, which can be converted into a scaled score. An average subject should obtain a scaled score of 10, with the standard deviation being 3 points. But the ‘normal’ range varies considerably with age; the performance subtests are particularly vulnerable to the effects of ageing. By correcting for age, age-scaled scores for each subtest can be derived.
The correlation between specific subtests and individual cognitive functions, and hence pathologies, is relatively poor, because many of the subtests tap several cognitive abilities simultaneously. For instance, Picture Arrangement is dependent upon visuoperceptual and planning abilities; therefore it is susceptible to both right hemisphere and frontal lobe damage.
A full account of the tests and their interpretation can be found in Neuropsychological Assessment (5th edition) by Lezak et al. (see ‘Selected Further Reading’). A brief description of each of the 10 core WAIS subtests is included here to aid clinicians with little or no experience of the test battery.
Verbal scales subtests
Perceptual reasoning subtests
Working memory subtests
Processing speed
Wechsler Memory Scale (WMS), Wechsler Memory Scale–Revised (WMS-R) and Wechsler Memory Scale-IV (WMS-IV) (Pearson Assessment)
The WMS was, for many years, the standard tool for the assessment of suspected memory disorders. It consisted of six subtests measuring orientation, mental control (attention), digit span, logical memory (story recall), verbal paired associate learning, and visual reproduction of geometrical figures. From these six subtests, a general memory quotient (MQ) could be obtained. The MQ was based on the sum of the raw scores. This total raw score was transformed with suitable age-adjustment to the MQ in such a way that it approximated to the full scale IQ of the WAIS. Thus an average person should obtain a full scale IQ of 100 and an MQ of 100, with the standard deviation of each being 15 points. A discrepancy between IQ and MQ of more than 15 points therefore indicates significant memory impairment. The major criticism of the WMS has been the bias towards verbal memory, the absence of delayed recall conditions for any of the subtests, and inclusion in the MQ score of subtests more dependent upon attentional processes (mental control and orientation) than upon memory per se.
The WMS-R was a considerable improvement. It incorporated two new visual memory tests (figural memory and visual paired associates), a new visual counterpart of digit span (visual memory span), a number of administration changes and, most importantly, delayed recall conditions for two of the verbal and two of the visual memory tests. As well as producing raw scores for each of the subtests, separate age-adjusted indices could be obtained for verbal, visual, and general memory, attention/concentration, and delayed recall.
The latest version of the WMS, the WMS-IV, introduced in 2009 again has significant changes to the previous version. In total 8 subtests were eliminated and 4 new subtests added: spatial addition, symbol span, design memory and general cognitive screener. Three older subtests were retained with modifications: logical memory, verbal paired associates and visual reproduction.
The WMS-IV is not appropriate tests for use at the bedside or in the clinic. Its administration requires expertise, and the scoring system is fairly complex. The digit span and logical memory subtests are the most easily adaptable. These provide good measures of attention and of verbal episodic memory, respectively. Everyday versions of these two subtests are described elsewhere (see ‘Digit Span’ and ‘Story Recall (Logical Memory)’ elsewhere in this chapter). The remainder of the subtests are described in the following list, to familiarize clinicians with their content, and thus to aid the interpretation of neuropsychological reports.
Western Aphasia Battery (WAB) (Pearson Assessment)
This instrument is similar to the longer and older Boston Diagnostic Aphasia Examination. It comprises four oral language subtests—spontaneous speech, auditory comprehension, repetition, and naming—which together yield five scores based on either a rating scale or conversion of summed item correct scores to a scale of 10. Each score can therefore be charted on a 10-point scale together to produce a profile of performance. An Aphasia Quotient can be calculated by multiplying each of the five scaled scores by two and summing. Normal (i.e. perfect) performance is set at 100. The profile of performance can be used to determine the patient’s diagnostic subtype according to classic descriptions of classic aphasia syndromes. In addition, tests of reading, writing, arithmetic, gestural praxis, construction, and reasoning are included to provide a comprehensive survey of communication abilities and related functions. The language portion of the test takes 1.5 hours to complete. As well as in patients with post-stroke aphasia, WAB data have been published in patients with Alzheimer’s disease, progressive aphasia, and vascular dementia.
The Wisconsin Card Sorting Test (WCST) (Pearson Assessment)
This widely used test was designed to study ‘abstract behaviour’ and ‘set-shifting ability’. It is sensitive to frontal lobe damage, particularly that involving the left dorsolateral area, and is failed by patients with dementing illnesses, particularly those of the subcortical type, but can be impaired in subjects with lesions elsewhere. The subject is given a pack of 64 cards on which are printed one to four symbols (triangle, star, cross, or circle) in one of four colours (see Fig. A.9). The subjects’ task is to place them, one by one, under four stimulus cards consisting of one red triangle, two green circles, three yellow squares, and four blue stars, according to a principle that the patient must deduce from the examiner’s responses. The examiner tells the subject if the choice was ‘right’ or ‘wrong’. For instance, if the principle is colour, the correct placement of the red card is under the red triangle, regardless of form of symbol or number. After 10 correct sorts, the examiner shifts the principle indicating the shift only in the changed pattern of ‘right’ or ‘wrong’ responses. The test begins with colour, then shifts to form, and then to number, before returning again to colour and so on. The most widely used scores are for number of categories achieved (maximum 6) and number of perseverative errors. Perseverative errors occur when the subject continues to sort according to a previously successful principle or, in the first series, when the subject persists in sorting on the basis of an initial erroneous guess.
The Modified Card Sorting Test (MCST) eliminates from the pack all cards that share more than one attribute with the stimulus card and the pack comprises only 48 cards. Whichever sorting dimension is chosen first is designated correct and more explicit shifting instructions are given. It is otherwise similar to the longer version. Further details are given in Neuropsychological Assessment (5th edition) by Lezak et al. (see ‘Selected Further Reading’).

Fig. A.9 Wisconsin Card Sorting Test.
Reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc. (PAR), 16204 North Florida Avenue, Lutz, Florida 33549, from the Wisconsin Card Sorting Test by David A. Grant., PhD and Esta A. Berg, PhD, Copyright 1981, 1993 by PAR. Further reproduction is prohibited without permission of PAR.
Addresses of Publishers
BrainMetric
52–13 Revere Rd
Drexel Hill, PA 19026
USA
http://www.brainmetric.com
Cambridge Cognition Ltd
Tunbridge Court
Tunbridge Lane
Bottisham
Cambridge CB25 9TU
UK
http://www.cantab.com
Pearson Assessment
Halley Court
Jordan Hill
Oxford, OX2 8EJ
UK
http://www.pearsonclinical.co.uk
PRO-ED, Inc.
8700 Shoal Creek Boulevard
Austin, TX 78751-6897
USA
http://www.proedinc.com
Psychological Assessment Resources, Inc. (PAR)
16204 North Florida Avenue
Lutz, FL 33549
USA
http://www.parinc.com